
Insomnia - How does it develop?
How does insomnia develop?
If you are going through a difficult time in your life or facing something stressful, it’s not uncommon to have problems with sleep. For most people, once the stressful situation passes the sleep problems also resolves. However, for about 10% of the population, the sleep problems can persist long after the initial trigger and can develop into chronic insomnia. Why does this happen? In this video, sleep physician Dr David Cunnington explains how chronic insomnia develops using what's known as the “3P model of insomnia.” Watch this video to learn more.
Dr. David Cunnington is a specialist sleep physician who delivers quality healthcare to clients with complex sleep problems. He promotes sleep health through education, research and advocacy. David is the co-director of Melbourne Sleep Disorders Centre, a multi-disciplinary sleep clinic for the diagnosis and treatment of sleep disorders. He has also developed a fantastic website called Sleep Hub, where an answer to almost any question on sleep can be found.
Like this article?
Grab a copy of our FREE eBook - A Short Guide to Better Sleep.
Looking for more information?
You can find more information about insomnia here. And you can learn more about the influence of thinking on sleep in the related articles When the mind won’t stop thinking, just sit back and watch and Are you stuck with insomnia, chronic fatigue or anxiety?
Video Transcript
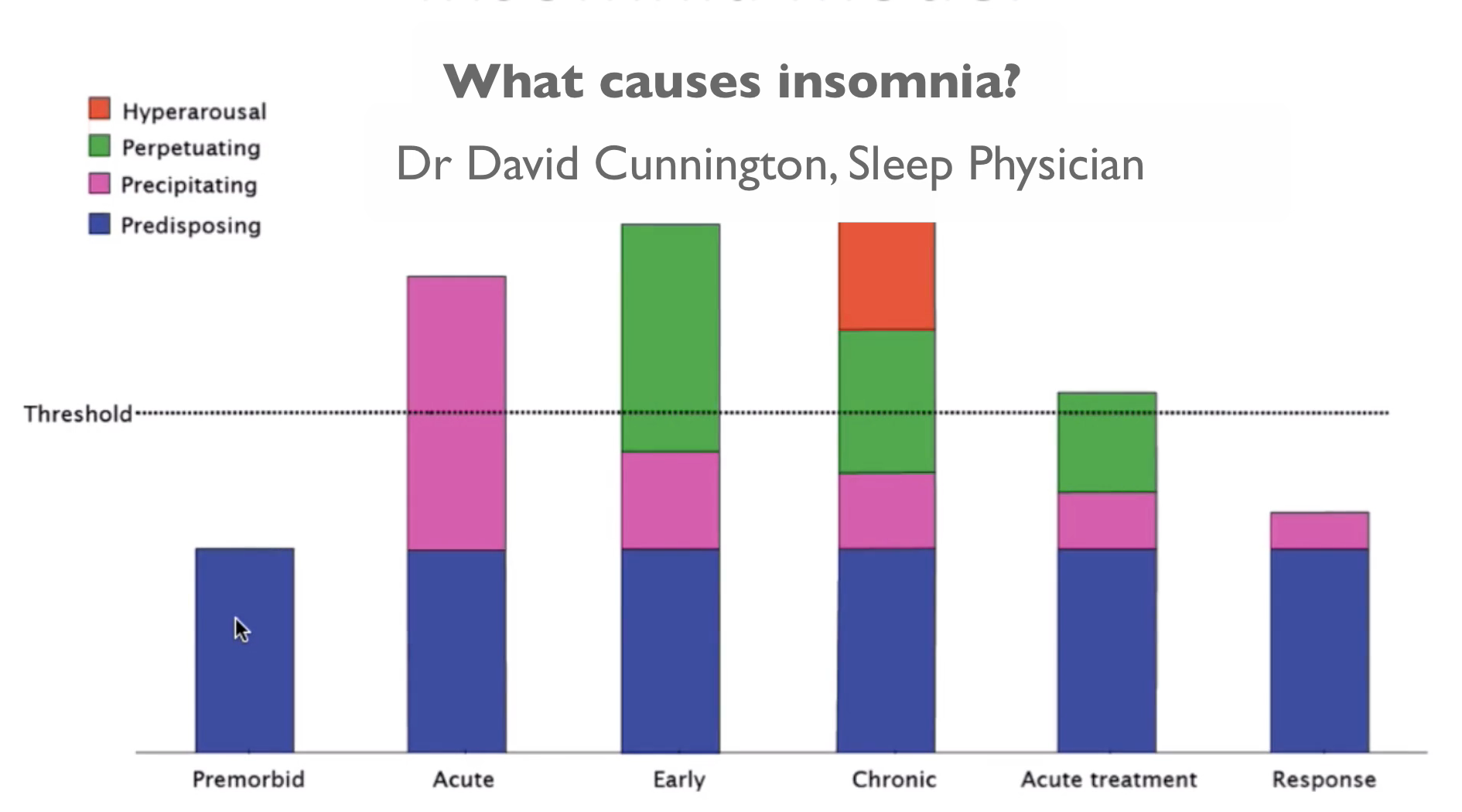
David: In understanding insomnia and the components to it, I find this model very helpful both to explain to people with insomnia the different parts we need to tackle and also when I’m talking with health professionals about insomnia and the different aspects of treatment we need to consider. This model was first conceptualised by Art Spielman in the 1980s and it has really stood the test of time in terms of our thinking about insomnia. Essentially the model looks at different components that can both predispose us to insomnia, can then trigger insomnia and perpetuate insomnia or keep it going.
Starting from the left side of the diagram if we look at this premorbid section here, what that really refers to is our biological predisposition to being good or bad sleepers. Some of us are good sleepers and some are not so good sleepers. But it would be very rare for any of us to be above the threshold for insomnia just based on our genetics.
Usually to develop insomnia, we need some sort of acute stress to come along. So it’s a set of circumstances that make us not sleep well for a short period of time while those circumstances are present – exams, job stress, work deadlines, stress in our relationships, family issues. Those are common examples and all of us will experience acute insomnia even a couple of times per year. But once that acute stress settles, then we usually settle back to this premorbid condition, our sort of genetic baseline and don’t have above threshold symptoms of insomnia.
However, if we’re under acute stress for long periods of time and therefore are having poor sleep for longer periods of time or there’s acute circumstances like illness or other things do go on for a long period of time and things don’t settle, we start to put into place coping strategies around sleep, represented by this green layer and those are things like going to bed earlier, sleeping in later, dropping out activities that we would normally do because we’re not sleeping well, using stimulants through the day to help us feel more alert because we’re feeling tired. These types of strategies actually just perpetuate the problem. They don’t help us sleep better. We put them in place because we think they’re going to. When they don’t work, we start to get this additional layer which is becoming anxious and frustrated around sleep itself. It can really get to the point where people recognise that a lot of their thinking during the day is about sleep and at night time they do get frustrated about not sleeping.
These are the four components that are all present when people come to see me when they’ve had chronic insomnia. By chronic insomnia, I mean insomnia that has been around for a couple of months or more. There’s usually something in terms of a biological predisposition or other physical and mental illness. There are circumstances that push them above the threshold for getting insomnia like all of us. They’ve usually got behaviours around sleep that are contributing to their problems like spending too long in bed, not getting out of bed when they’re awake and spending too much time awake in bed. They’re often anxious or frustrated about their sleep. So these are the four areas that we need to tackle in planning a management strategy for insomnia.
This really highlights why medications aren’t the answer for chronic insomnia because arguably medications really are acting on this biological component but they’re often not the parts that are pushing people above the threshold for getting insomnia. That’s where the role of psychology-based treatments comes in, looking at people’s thinking around sleep and changing their thinking, looking at people’s behaviours around sleep and changing their behaviours.
That’s what we try to do with the psychology-based treatment, cognitive behavioural therapy for insomnia. Over time, we aim to get people thinking about sleep in a way that they were before, usually not thinking about it at all. So we’re aiming to get to this point. We’re no longer anxious about sleep and most of the behaviours around sleep have improved. Still getting some insomnia but a lot better than before. Then over time as people get more confident in that and their thinking about sleep continues to settle and their behaviours around sleep settle back to a more normal pattern, this is the point we aim to get people to, at the right side of the graph where they’ve still got those biological factors that are going to contribute to being a good or bad sleeper.
They’re still a bit sensitive about things coming up in the diary that are going to be threats to sleep like international travel or another deadline or more exams. But their behaviour around sleep is good and they’re thinking about sleep is good.
If we can get people to this point, then even if they do have a relapse of their symptoms, if we’ve up-skilled them in managing their behaviour and thinking about sleep, they don’t go back into the situation because even if they do get an acute insomnia, they know how to manage their behaviour and thinking and can settle back down to this pattern.
I hope that has given you an idea of how we conceptualise insomnia. I find this model really helpful in practice as it always guides me in terms of what I can do in treating people, in looking at those four domains of thinking around sleep, behaviour around sleep, how people respond to threats to sleep or challenges to sleep and things with their underlying biology and physical and mental illness that may be contributing to sleep problems.






